03 Jun PCOS Has Been Renamed PMOS: An Aesthetic Doctor Explains What This Means for Your Skin
Polycystic ovary syndrome, better known as PCOS, was renamed PMOS, or polyendocrine metabolic ovarian syndrome in May 2026. This change reflects a long overdue name change, which caused many patients to misunderstand that polycystic ovarian syndrome was simply a condition of ovarian cysts, when PCOS, in fact, was a broader endocrine and metabolic condition that can affect periods, ovulation, fertility, insulin resistance, cardiometabolic health, skin and hair1,2. PMOS is a more accurate description of this condition.
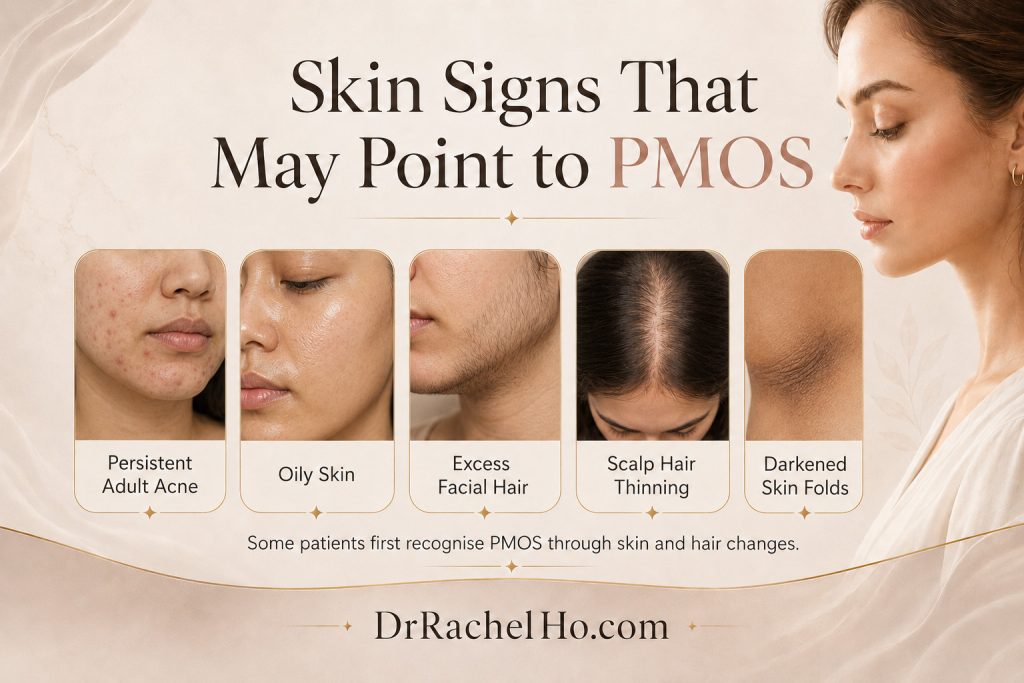
As an aesthetic doctor, I find this change to be very significant because some patients may first recognise PCOS or PMOS through their skin. Persistent adult acne, oily skin, excess facial hair, scalp hair thinning and darkened skin folds may be the initial clues that bring someone to a skin doctor before they see a gynaecologist or endocrinologist.
View this post on Instagram
What was PCOS?
Polycystic ovarian syndrome was traditionally described as a condition involving ovulatory dysfunction, androgen excess and polycystic ovarian morphology. The Rotterdam criteria supports diagnosis of PCOS at least two of these three features are present and after other causes are excluded: irregular ovulation or menstrual cycles, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology on ultrasound3,4.
PMOS stands for Polyendocrine Metabolic Ovarian Syndrome
What does PMOS mean and why was PCOS renamed as PMOS?
PMOS stands for polyendocrine metabolic ovarian syndrome. This new terminology is a more accurate reflection of the actual condition, which involves multiple hormonal and metabolic pathways, including androgen excess, ovulatory dysfunction and insulin resistance, which can affect periods, fertility, cardiometabolic health, skin and hair. The 2026 international consensus behind the name change stated that the term PCOS was inaccurate because it implied pathological ovarian cysts and obscured the condition’s endocrine and metabolic features.
Why the name change from PCOS to PMOS is important for patients
The name PCOS has contributed to stigma and confusion for patients for many years. Some patients were told they could not have PCOS because they did not have ovarian cysts. Or, they were reassured because their periods were regular, even though they had acne, facial hair, hair thinning or metabolic signs. Each word in PMOS carries a deliberate meaning1,2:
- Polyendocrine: Recognises that the condition involves multiple interacting hormonal systems, including insulin, androgens, and neuroendocrine hormones.
- Metabolic: Acknowledges the metabolic dysfunction of the condition, including insulin resistance, dyslipidaemia, and elevated risk of type 2 diabetes and cardiovascular disease.
- Ovarian: Retains the ovarian component because ovarian dysfunction, including altered folliculogenesis and androgen production, remains a key feature of the condition.
- Syndrome: Preserved to reflect the spectrum of features and phenotypes that characterise the condition rather than implying a single disease entity.
PMOS makes the condition easier to understand as a systemic condition, rather than an isolated ovarian syndrome. This also explains why care for PMOS or PCOS can involve several specialties, including dermatology, gynaecology, endocrinology and primary care.
Skin signs of PCOS or PMOS include oily skin, acne, hirsutism, acanthosis nigricans and seborrhoeic dermatitis
How PMOS can affect the skin
PMOSis highly relevant to dermatology because manifestations in the skin are often the first presenting signs of women with PCOS2. The skin signs of PCOS or PMOS are mainly linked to androgen excess and insulin resistance. The most common dermatological features include acne, oily skin, hirsutism, female pattern hair loss and acanthosis nigricans5,6.
Acne in PMOS
Acne in PMOS typically presents along the lower face: the jawline, chin, neck, and occasionally the upper chest and back. The lesions tend to be deep, cystic, and cyclically worse in the days before menstruation. They are resistant to standard topical treatments because topical products address the follicular environment but cannot lower systemic androgen levels in PMOS6,7.
In patients with Fitzpatrick skin types III to VI, which represents the majority of the Singapore population, acne in PMOS frequently leaves behind significant post-inflammatory hyperpigmentation. The combination of active acne and persistent dark marks creates a cumulative skin burden and requires a treatment strategy that addresses both the hormonal contributions and the pigmentary consequence6,7.
Related blogpost:
Adult Female Acne: A Doctor Explains
Cycle Sync Skincare for Menstrual Acne
Hirsutism in PMOS
Excess androgen activity affects the hair follicle directly, producing hirsutism (increased terminal hair in androgen-sensitive areas including the face, chest, and abdomen) and paradoxically contributing to androgenic alopecia (temporal or diffuse thinning of scalp hair)8.
Acanthosis nigricans in PMOS
Insulin resistance, a central metabolic feature of PMOS, drives the velvety, hyperpigmented thickening that appears in skin folds including the neck, axillae, and groin. Elevated insulin levels stimulate insulin-like growth factor receptors on keratinocytes, promoting epidermal hyperplasia and melanin production9. When I see acanthosis nigricans in a young woman presenting with acne, I consider it a significant clinical signal pointing toward insulin resistance and, very often, PMOS.
Seborrhoea and Scalp Conditions in PMOS
Increased sebum production driven by androgenic stimulation of sebaceous glands affects the scalp as well as the face, contributing to seborrhoeic dermatitis and oily scalp conditions8. Understanding these as manifestations of the same androgen excess driving facial acne allows for more targeted treatment planning.
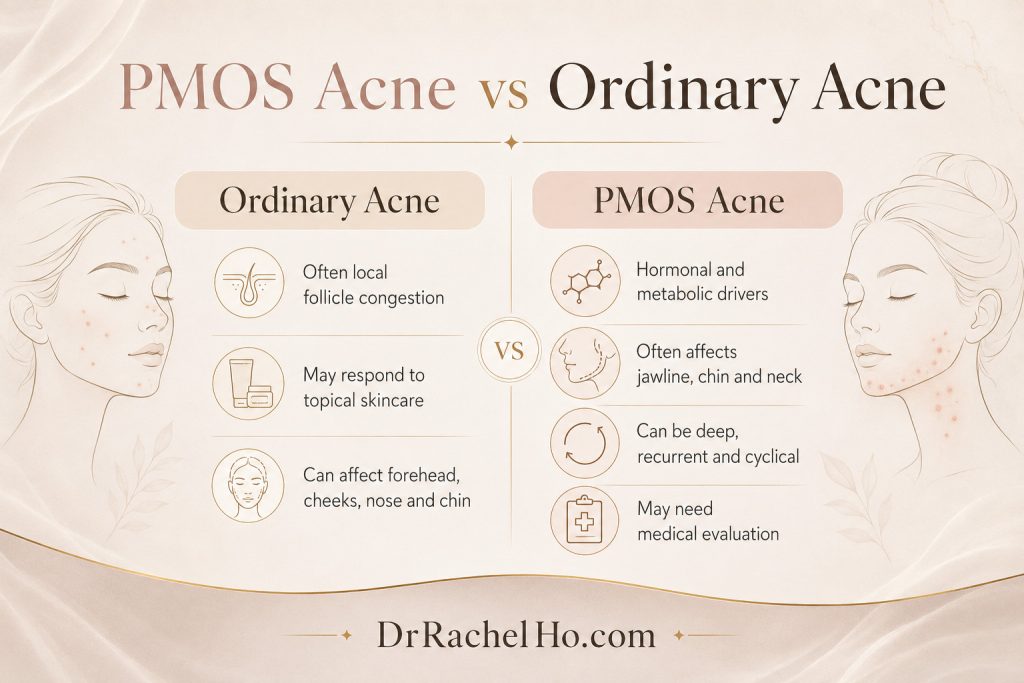
How does PMOS/ PCOS acne differ from ordinary acne?
Why PMOS acne is different from ordinary acne
PMOS acne tends to be more severe than non-PCOS acne10. While acne distribution is similar to the general population in many PMOS patients, in those with concurrent hirsutism, acne most commonly affects the chin, jawline, cheeks, and trunk—a more androgen-driven pattern12.
PCOS acne results from both hyperandrogenism and hyperinsulinemia, whereas ordinary acne primarily involves local pilosebaceous factors12,13. Hyperinsulinemia stimulates androgen secretion from the ovaries and adrenal glands. This suppresses sex hormone-binding globulin (SHBG) synthesis, increasing free, biologically-active androgens. PMOS patients with acne also tend to have significantly higher testosterone levels and raised LH/FSH ratios13.
Patients with POMS often respond poorly to first-line topical treatments (explained in 5 Skincare Ingredients for Acne & Acne Prone Skin) that typically work for ordinary acne and often require systemic treatments including hormonal treatments, oral antibiotics, or isotretinoin to achieve control11,14.
Dr Rachel’s takeaway on the name change from PCOS to PMOS
The renaming of PCOS to PMOS is a helpful correction of an endocrine and metabolic syndrome that affects the skin. Acne, oily skin, facial hair growth, scalp hair thinning and darkened skin folds are some of the signs of PMOS that patients may first present to the doctor with.
If you have been dealing with persistent hormonal acne, unexplained hair thinning, or acanthosis nigricans and have never had a hormonal evaluation, this is the moment to ask for one. These are skin signals that are suggestive of PMOS, and you can benefit from a hormonal evaluation.
I will be watching how the clinical guidelines evolve through the PMOS transition period, particularly the 2028 international guideline update, and will update this post accordingly as new evidence on subtypes and management emerges.
References
- Polyendocrine Metabolic Ovarian Syndrome: New name to improve diagnosis and care of condition affecting 170 million women worldwide. Endocrine Society. 2026.
- Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome. Teede HJ, et al. The Lancet. 2026.
- Recommendations From the 2023 International Evidence Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Teede HJ, et al. Journal of Clinical Endocrinology and Metabolism. 2023. Volume 108, Issue 10.
- International Evidence Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome 2023. Monash University and International PCOS Network. 2023.
- Update on Management of Polycystic Ovarian Syndrome for Dermatologists. Gainder S, Sharma B. Indian Dermatology Online Journal. 2019. Volume 10, Issue 2.
- Cutaneous Findings Associated With Polycystic Ovary Syndrome. Schmidt TH, et al. JAMA Dermatology. 2016. Volume 152, Issue 4.
- Cutaneous Manifestations and Hormonal Changes Among Polycystic Ovary Syndrome Patients at a Tertiary Care Center. Aljefri et al. Cureus. 2021 Dec 22;13(12):e20593.
- A narrative review on cutaneous manifestations in polycystic ovary syndrome: pathophysiology, diagnosis, management, and psychosocial impact. Farhan et al. Ann Med Surg (Lond). 2025 Mar 28;87(5):2804–2811.
- Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Escobar-Morreale. Nat Rev Endocrinol. 2018 May;14(5):270-284.
- Characterizing clinical and hormonal profiles of acne in north African women with polycystic ovary syndrome. Abdessalem et al. Arch Dermatol Res. 2024 Oct 26;316(10):711.
- Comprehensive transition of care for polycystic ovary syndrome from adolescence to adulthood. Simon et al. Lancet Child Adolesc Health. 2024 Jun;8(6):443-455.
- The Association of Glucose Metabolism Disorders and Acne in Women With Polycystic Ovary Syndrome (PCOS). Damoulaki et al. In Vivo. 2025 Jul-Aug;39(4):2219-2227.
- Metformin versus the combined oral contraceptive pill for hirsutism, acne, and menstrual pattern in polycystic ovary syndrome. Fraison et al.The Cochrane Database of Systematic Reviews. 2020.
- Management of Acne Vulgaris: A Review. Eichenfield et al. JAMA. 2021 Nov 23;326(20):2055-2067.
No Comments