15 Mar Keratosis Pilaris (Chicken Skin) in Singapore: Doctor’s Guide
What Is Keratosis Pilaris or Chicken Skin?
Keratosis pilaris (KP) is a benign, chronic disorder of follicular keratinisation. It is characterised by the accumulation of keratin within the infundibulum of the hair follicle, leading to a plug that occludes the follicular opening and produces the distinctive rough, papular texture associated with the condition, giving rise to an appearance of chicken skin. Keratosis pilaris tends to affect the upper and lower limbs;
Keratosis pilaris is common; and studies estimate a prevalence of approximately 40% of adults and up to 50 to 80% in adolescents1. In Singapore, KP is frequently identified as a concomitant finding in patients presenting with atopic dermatitis: a local study at the National Skin Centre found keratosis pilaris in 13% of Singapore schoolchildren with atopic dermatitis2 .
Related blogposts:
Eczema: Causes, Symptoms & Treatments Explained
How to Repair Your Skin Barrier
Keratosis pilaris usually appears in early childhood and progresses, becoming most apparent in early adulthood3. This condition tends to follow a chronic relapsing course, but some patients may show improvement in adulthood.

How chicken skin or keratosis pilaris forms
What Does Keratosis Pilaris Look Like on Asian Skin
The clinical presentation for keratosis pilaris differs for patients with different skin tones.
In patients with fair skin (Fitzpatrick skin types I to II), KP typically appears as small, rough, skin-coloured or slightly red papules arranged in a follicular pattern on the outer upper arms, thighs, and buttocks4,5. Sometimes, there is mild surrounding pinkness or erythema4,5.
In patients with darker skin (Fitzpatrick skin types III to V), which encompasses the majority of Singaporeans, the presentation can look different:
• The papules are more likely to be surrounded by brownish or grey-brown discolouration rather than redness, as darker skin types produce post-inflammatory hyperpigmentation (PIH) more readily in response to follicular inflammation6,7.
• The overall appearance can resemble scattered dark spots or tiny blackheads covering the affected area, rather than the red or pink bumps commonly depicted in textbooks6,7.
• Textural roughness may be the more prominent complaint, with pigmentation around the follicles adding a second layer of cosmetic concern on top of the physical bumps.
Related blogpost:
Hyperpigmentation Disorders: Causes, Types, Treatments
The most commonly affected sites across all ethnicities are the posterolateral upper arms, anterior thighs, buttocks, and cheeks. When KP affects the cheeks, it is termed keratosis pilaris rubra faceii (KPRF) and can be mistaken for acne or rosacea, particularly in patients with significant perifollicular pigmentation rather than erythema8.
Related blogposts:
Hyperpigmentation Disorders: Causes, Types, Treatments
Adult Female Acne: A Doctor Explains (Singapore)
Cycle Sync Skincare for Menstrual Acne
Rosacea: Symptoms, Triggers, Skincare and Treatments
5 Skin Care Tips for Sensitive Skin and Rosacea
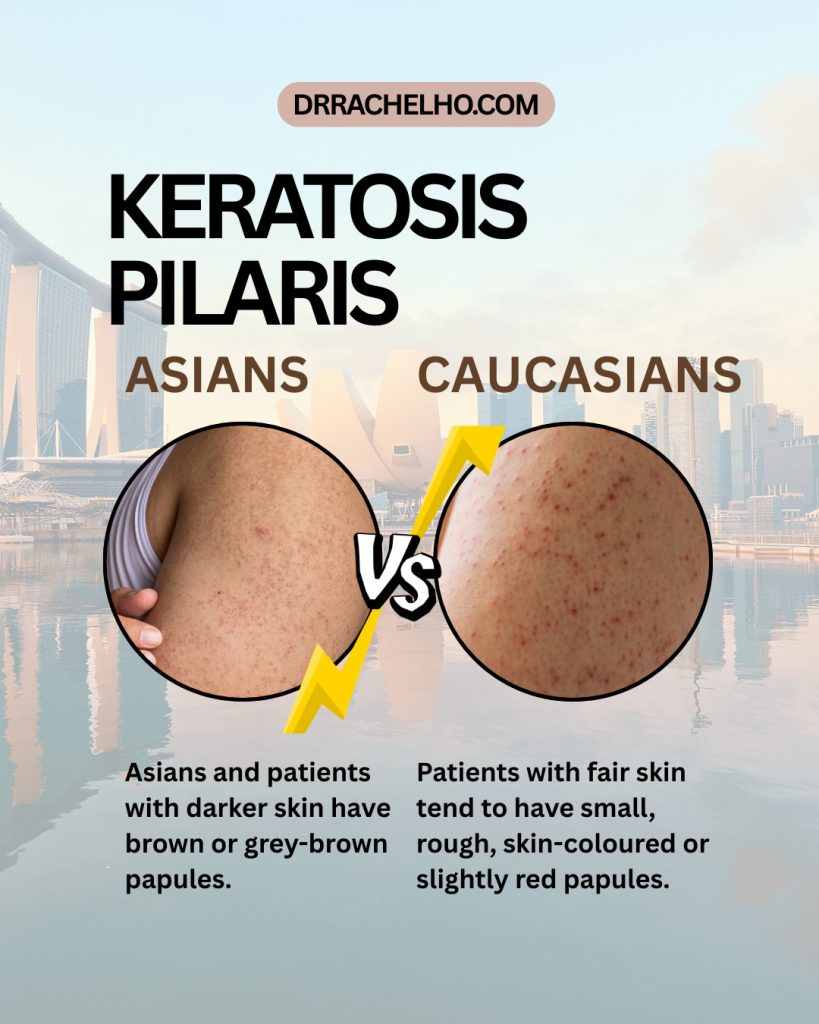
Keratosis pilaris or chicken skin tends to look different in Asians compared to Caucasians.
Risk Factors and Why KP Develops
Genetics and the Singapore connection
Although keratosis pilaris is a common condition, the exact cause remains unknown. Keratosis pilaris can be transmitted by an autosomal dominant mode of inheritance.
At a molecular level, KP is closely linked to filaggrin (FLG) gene mutations, with approximately 35% of KP patients carrying filaggrin null mutations9. Filaggrin is a structural protein critical to normal keratinocyte differentiation and the formation of the skin barrier. Its deficiency leads to aberrant keratinisation within the follicular infundibulum, impaired stratum corneum hydration, and increased transepidermal water loss, all of which contribute to the presentation of keratosis pilaris.
Importantly, the specific filaggrin mutations observed in Singaporean and Asian patients differ from those identified in European populations. While European populations predominantly carry FLG mutations R501X and 2282del4, the Singaporean Chinese population carries a distinct spectrum of seven FLG null mutations, including 3321delA, 6950_6957del8, S1515X, S2706X, Q2417X, E2422X, and G323X, which together, account for approximately 80% of the FLG mutation spectrum in this population10,11 Malay and Indian Singaporeans carry their own ethnicity-specific FLG mutation profiles8. This population-specific genetic difference means that research conducted in European patients may not directly translate to Singapore and other Asian populations.
Atopic conditions
KP is strongly associated with atopic dermatitis (AD) and ichthyosis vulgaris, both of which share the filaggrin deficiency pathway. Atopic dermatitis is highly prevalent in Singapore: a national study found a high prevalence of AD in Singapore schoolchildren, comparable to rates in developed Western countries, with heat and sweating identified as common aggravating factors2. The same study identified keratosis pilaris in 13% of affected children, underscoring the clinical overlap between these conditions in the local population.
An evidence based treatment guide to keratosis pilaris or chicken skin in Singapore
Treatment Options for Chicken Skin Tailored to Asian Skin
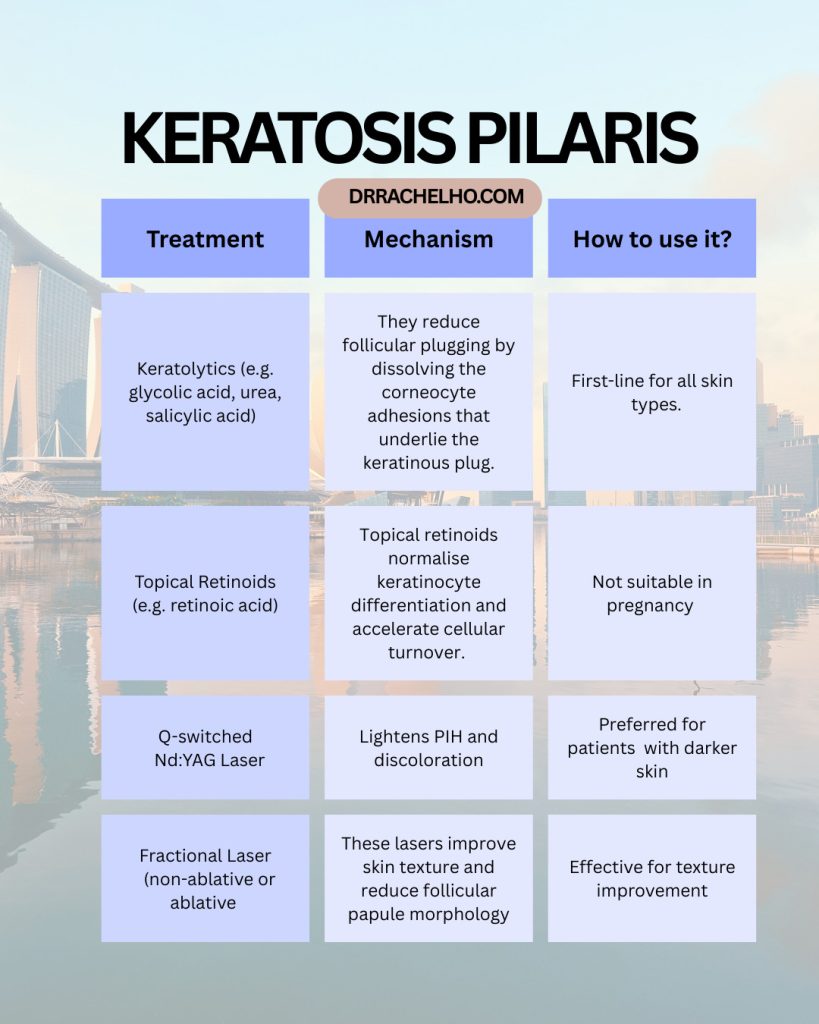
Keratosis pilaris does not cause symptoms for most people and can improve without treatments4. he main aim of treatment for keratosis pilaris is to reduce follicular plugging and address associated pigmentation. Treatment options include:
1. Topical Keratolytics
Keratolytics are first-line treatment for all patients7. They reduce follicular plugging by dissolving the corneocyte adhesions that underlie the keratinous plug. Examples of keratolytics include glycolic acid, urea and lactic acid.
Related blogposts:
A Complete Guide to Acids in Skincare
2. Topical Retinoids
Topical retinoids normalise keratinocyte differentiation and accelerate cellular turnover14. Tretinoin at 0.025 to 0.05% and adapalene 0.1% are suitable options, with adapalene generally better tolerated by patients with sensitive or reactive skin.
Related blogpost:
How Does Retinol Work? Retinol Explained Simply
3. Laser and Energy-Based Treatments
For patients in whom topical treatments produce insufficient improvement, laser-based interventions are a well-evidenced option. The Q-switched Nd:YAG laser at 1064 nm is the preferred laser modality for KP in Asian skin. Its longer wavelength penetrates deeper into the dermis with less epidermal melanin absorption, reducing the risk of PIH compared to shorter-wavelength lasers. A study evaluated Q-switched Nd:YAG laser at 1064 nm with low fluence in ten Asian patients with pigmented KP, and demonstrated clinical improvement in all patients with minimal adverse effects13. In a broader review of KP treatment, Nd:YAG laser was identified as a preferred option across skin types due to its relatively favourable side effect profile15.
Related blogposts:
10 Things to Know Before Having Lasers
4. Fractional Laser
Fractional CO2 lasers improve skin texture and reduce follicular papule morphology16.
Doctor’s Takeaway for Keratosis Pilaris
KP or chicken skin is one common skin concern I address in my clinic, and it is one where I consistently see a gap between what patients have been told and what is actually achievable.
In Singaporean patients, KP frequently presents with pigmentation rather than redness, which means it is often confused with other conditions. Getting that diagnostic step right is the foundation of everything else.
Secondly, the treatments that work well for fair skin in European studies cannot simply be applied to Chinese, Malay, or Indian skin at the same settings. The risk of making existing pigmentation worse through poorly chosen or aggressively delivered treatment is real, and it is avoidable with the right protocol.
For patients whose KP has not responded adequately to a structured topical regimen, laser-based and energy-based options exist that are appropriate for Asian skin phototypes when selected and delivered correctly. The Q-switched laser has the most evidence in Asian patients with pigmented KP, and microneedling with adjuncts is a useful option for those who prefer to avoid laser-related downtime or carry high PIH risk.
References
1. Treatment of keratosis pilaris and its variants: a systematic review. Maghfour et al. J Dermatolog Treat. 2022 May;33(3):1231-1242.
2. The prevalence and descriptive epidemiology of atopic dermatitis in Singapore school children. Tay et al. Br J Dermatol. 2002 Jan;146(1):101-6.
3. Keratosis Pilaris. Pennycook et al. StatPearls [Internet].
4. Keratosis pilaris rubra with mucin deposition. Hosking et al. J Cutan Pathol. 2018 Dec;45(12):958-961.
5. Skin diseases associated with atopic dermatitis. Fenner and Silverberg. Clin Dermatol. 2018 Sep-Oct;36(5):631-640.
6. Keratosis pilaris rubra: a common but underrecognized condition. Marqueling et al. Arch Dermatol. 2006 Dec;142(12):1611-6.
7. Keratosis pilaris: a systematic review of the literature and strategies for optimal treatment. Beyron. Eur J Dermatol. 2025 Oct 1;35(5):387-393.
8. Keratosis pilaris atrophicans faciei: An observational, descriptive, retrospective clinical study. Fekete. Exp Ther Med. 2021 Sep 20;22(5):1331.
9. Sebaceous gland, hair shaft, and epidermal barrier abnormalities in keratosis pilaris with and without filaggrin deficiency. Gruber et al. Am J Pathol. 2015 Apr;185(4):1012-21.
10. Wide spectrum of filaggrin-null mutations in atopic dermatitis highlights differences between Singaporean Chinese and European populations. Chen et al. Br J Dermatol. 2011 Jul;165(1):106-14.
11. Comprehensive analysis of the gene encoding filaggrin uncovers prevalent and rare mutations in ichthyosis vulgaris and atopic eczema Sandilands et al. Nat Genet. 2007 May;39(5):650-4.
12. Array-based sequencing of filaggrin gene for comprehensive detection of disease-associated variants. Wong et al. J Allergy Clin Immunol. 2018 Feb;141(2):814-816.
13. Treatment of pigmented keratosis pilaris in Asian patients with a novel Q-switched Nd:YAG laser. Kim. J Cosmet Laser Ther. 2011 Jun;13(3):120-2
14. Topical tretinoin (retinoic acid) treatment of hyperpigmented lesions associated with photoaging in Chinese and Japanese patients: a vehicle-controlled trial. Griffiths et al. J Am Acad Dermatol. 1994 Jan;30(1):76-84.
15. Keratosis Pilaris Unveiled: Insights into its Origin, Management Strategies and Research Frontiers. Kaur et al. Indian J Dermatol. 2025 Sep-Oct;70(5):267-274.
16. Fractional Carbon Dioxide Laser for Keratosis Pilaris: A Single-Blind, Randomized, Comparative Study. Vachiramon et al. Biomed Res Int. 2016 May 9;2016:1928540.
No Comments